Chylothorax is a rare disease characterized by the accumulation of chyle (a milky bodily fluid) in the pleural cavity. Although uncommon, it can lead to severe complications and death. A thorough understanding of the primary causes of chylothorax is crucial for timely intervention, prevention of respiratory distress, malnutrition, and immunological issues due to the loss of lymphocytes[1], thereby facilitating effective patient recovery.
How Chylothorax Develops
Chylothorax is characterized by the accumulation of chyle within the pleural cavity. The term “chyle” is derived from the Greek word chylos, meaning “juice.”
Composition and appearance of chyle:
1. Chyle is a milky-white fluid formed by the intestinal lymphatic system during fat digestion. It is rich in triglycerides, lymphocytes, immunoglobulins, and fat-soluble vitamins[2].
2. Macroscopically, chyle usually appears milky white, but it may sometimes appear serous (especially in patients who are fasting or have reduced lipid intake, such as postoperatively) or blood-stained (particularly following trauma). Other reported appearances include serosanguineous, yellow, and green coloured fluid[2].
Chyle primarily originates from the process of fat digestion in the small intestine. It is collected by the intestinal lymphatic vessels and transported to the cisterna chyli in the abdomen, from which it is transported upward through the thoracic duct into the thoracic cavity. Damage or rupture of the thoracic duct or its branches due to various causes can result in the development of chylothorax.
Key anatomical structures:
-
Thoracic duct: The largest lymphatic vessel in the human body and also the main collecting channel of the lymphatic system. It originates from the cisterna chyli in the abdomen and measures approximately 35-46 cm in length[2].
-
Cisterna chyli: A saclike lymphatic structure located in the retroperitoneal space, formed by the convergence of major abdominal lymphatic vessels. It serves as the starting point of the thoracic duct and collects chyle from the intestinal lymphatics.
Incidence and Clinical Presentation of Chylothorax
Chylothorax is relatively rare, accounting for approximately 3% of all cases of pleural effusion[2].
The clinical manifestations of chylothorax are diverse and closely related to both the underlying cause and the rate at which chyle accumulates within the pleural cavity.
In addition to symptoms caused by the primary disease, patients with chylothorax may experience cough, sputum production, chest tightness, shortness of breath, and palpitations. If accompanied by infection, additional symptoms such as fever, chills, and chest pain may also occur. When the effusion volume is large, it can lead to respiratory distress or even respiratory failure. Furthermore, hemorrhagic chylothorax may cause symptoms of anemia or hypovolemic shock, including fatigue, thirst, and dizziness, and may also result in weight loss, malnutrition, immunodeficiency (weakened immunity), and edema.
The Primary Causes of Chylothorax
The causes of chylothorax can be primarily classified into two major categories: traumatic and non-traumatic. Accurate identification of the underlying cause is the first step in the successful management of chylothorax.
1. Traumatic Chylothorax
Traumatic chylothorax is the most common type[1,2]. It can be further subdivided into iatrogenic and non-iatrogenic categories.
Iatrogenic refers to injury associated with medical procedures or surgery, while non-iatrogenic is typically caused by factors such as accidental trauma.
- Iatrogenic Injury: Postoperative chylothorax is the most common type of chylothorax in clinical practice. Procedures prone to causing chylothorax include esophagostomy, lung cancer resection, coronary artery bypass surgery, thoracic aneurysm repair, or cardio-pulmonary transplantation.
- Non-Iatrogenic Trauma: This includes penetrating injuries, such as gunshot or knife wounds to the chest. Blunt trauma from vehicular accidents can also lead to thoracic duct rupture. Additionally, chylothorax has been reported following blast injuries and even minor events such as coughing or sneezing.
2. Nontraumatic (Spontaneous) Chylothorax
Non-traumatic chylothorax is uncommon and has a broad differential diagnosis. It can be caused by the following factors:
-
Congenital chylothorax: The cause of congenital chylothorax remains unclear, but it may be associated with genetic mutations or congenital abnormalities of the lymphatic system.
-
Neoplastic chylothorax (most common): Lymphoma (especially non-Hodgkin lymphoma, accounting for approximately 70% of malignant cases), lung cancer, esophageal cancer, metastatic cancer, etc., are all associated with chylothorax.
-
Systemic diseases: Such as systemic lupus erythematosus and Behçet's disease.
-
Infectious chylothorax: Tuberculous lymphadenitis is the most common, with other infectious causes including aortitis, histoplasmosis, and filariasis.
-
More rare causes of chylothorax reported: Castleman disease, sarcoidosis, yellow nail syndrome, Down syndrome, Noonan syndrome, Waldenström macroglobulinemia, venous thrombosis, amyloidosis, thoracic radiation, and goiter.
-
Parenteral nutrition therapy is also associated with chylothorax.
*Additionally, idiopathic chylothorax exists.
Approximately 10% of chylothorax cases, even after extensive evaluation, cannot be identified as having traumatic or pathological causes and are classified as idiopathic chylothorax. The etiology remains unclear.
Diagnosis of Chylothorax
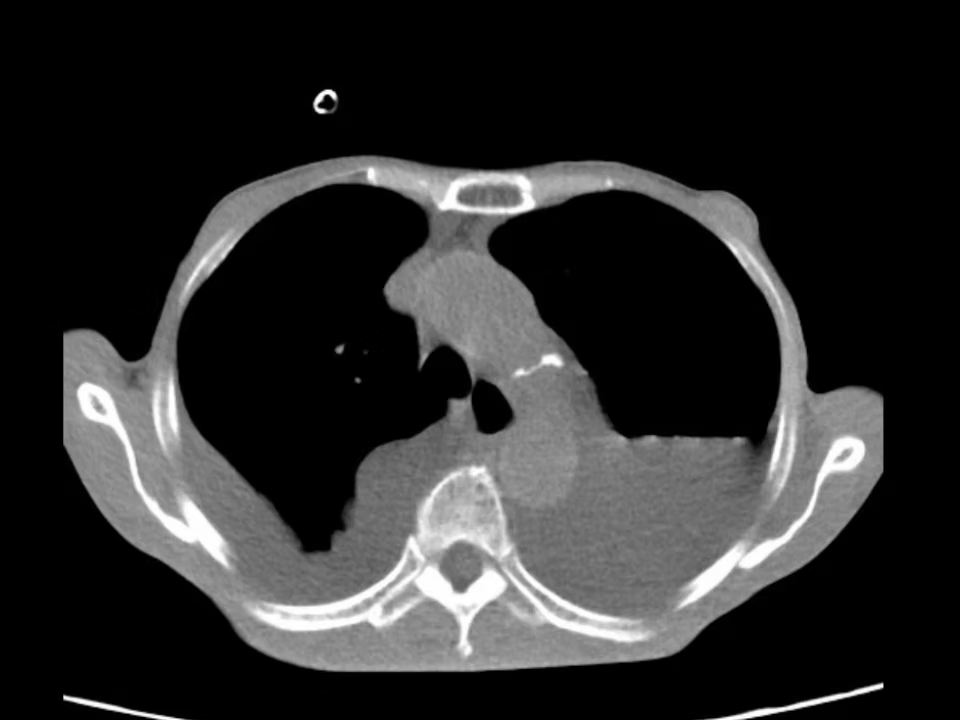
Analysis of pleural fluid is central to the diagnosis of chylothorax, and various thoracic imaging examinations can provide supplementary diagnostic information.
The key purpose of these examinations is to identify the underlying cause, with particular emphasis on ruling out secondary chylothorax caused by common conditions such as tumors.
Common diagnostic methods include:
Thoracentesis, Chest X-rays, Chest CT, Thoracic Utrasound, Chest MRI (magnetic resonance imaging), Conventional Lymphangiography, Nuclear Lymphoscintigraphy.
Modern Management and Treatment of Chylothorax
The treatment goals for chylothorax are to control the accumulation of chyle, relieve symptoms, and address the underlying cause. Therapeutic approaches are divided into two main categories: conservative management and surgical intervention, with the specific choice typically determined by the cause of the chylothorax and the severity of the condition.
1) Conservative Management
1. Diet and Nutritional Support
-
Low-fat or fat-free diet, supplemented with albumin to reduce lymphatic production.
-
Parenteral nutrition support when necessary, including administration of plasma, albumin, and amino acids.
2. Symptom Relief
-
Thoracentesis for pleural fluid aspiration and drainage.
3. Pharmacologic Therapy
-
Reports indicate that somatostatin and octreotide can reduce chyle production[1,2].
4. Provide or Intensify Treatment Targeting the Underlying Causes
-
E.g, for chylothorax caused by malignancy, intensify anticancer therapy such as radiotherapy and chemotherapy.
2) Surgical Interventions
Surgical management is indicated when conservative measures prove ineffective.
Common surgical techniques include:
1. Thoracic Duct Ligation
2. Pleurodesis
3. Thoracic Duct Embolization and Disruption
Case (Comprehensive Treatment Approach):
Expert Care with ICWS
Chylothorax, a rare and complex condition, requires specialized expertise and multidisciplinary team collaboration. ICWS is dedicated to providing advanced diagnostic and therapeutic solutions for patients worldwide. Based on a patient-centered treatment approach, ICWS offers comprehensive support for individuals with thoracic diseases.
Main references for the article:
[1] Rudrappa, M., & Paul, M. (2024, July 28). Chylothorax. StatPearls - NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK459206/
[2] Bhatnagar, M., Fisher, A., Ramsaroop, S., Carter, A., & Pippard, B. (2024). Chylothorax: pathophysiology, diagnosis, and management—a comprehensive review. Journal of Thoracic Disease, 16(2), 1645–1661. https://doi.org/10.21037/jtd-23-1636